
Demonstrated progression-free survival (PFS) in metastatic renal cell carcinoma (mRCC), including long-term follow up

Demonstrated progression-free survival (PFS) in metastatic renal cell carcinoma (mRCC), including long-term follow up
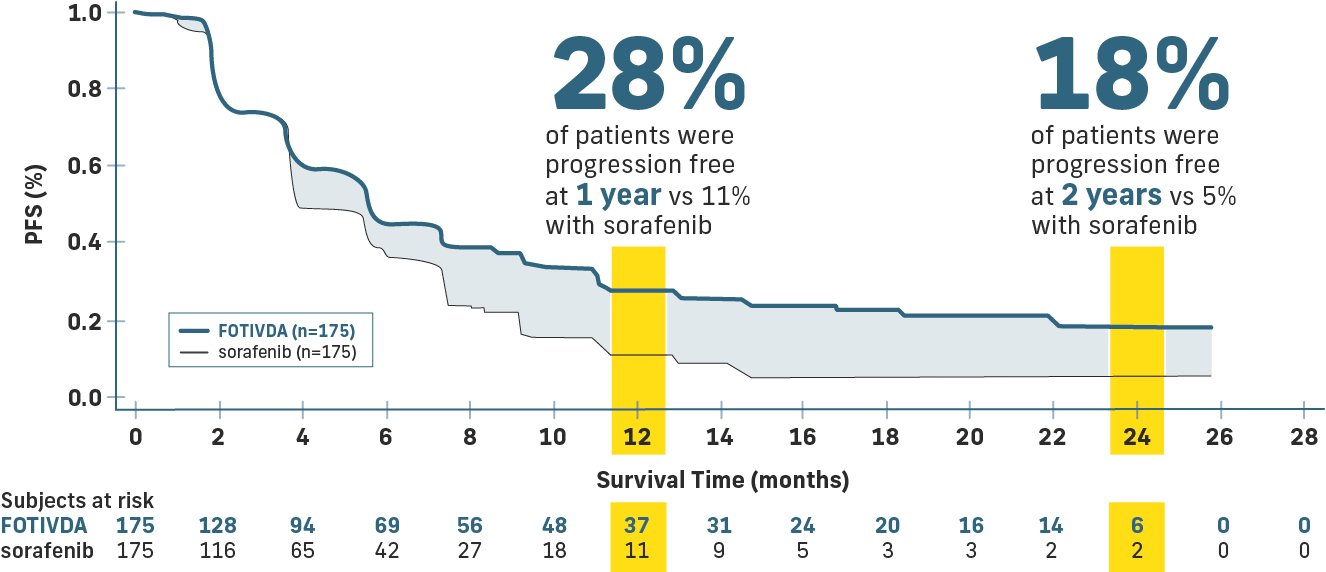
FOTIVDA: Superior results vs sorafenib1,2
- 44% improvement in median PFS (5.6 months vs 3.9 months)
- 27% reduction in risk of death or progression (HR=0.73)
mPFS: 5.6 months with FOTIVDA vs 3.9 months with sorafenib (HR=0.73 [95% CI: 0.56, 0.95], P=0.02)
FOTIVDA: Long-term PFS from 5-year follow-up3
- Landmark data show PFS rates are consistently higher with FOTIVDA vs sorafenib, with 12% vs 2% and 8% vs 0% at 3 and 4 years, respectively
Progression Free
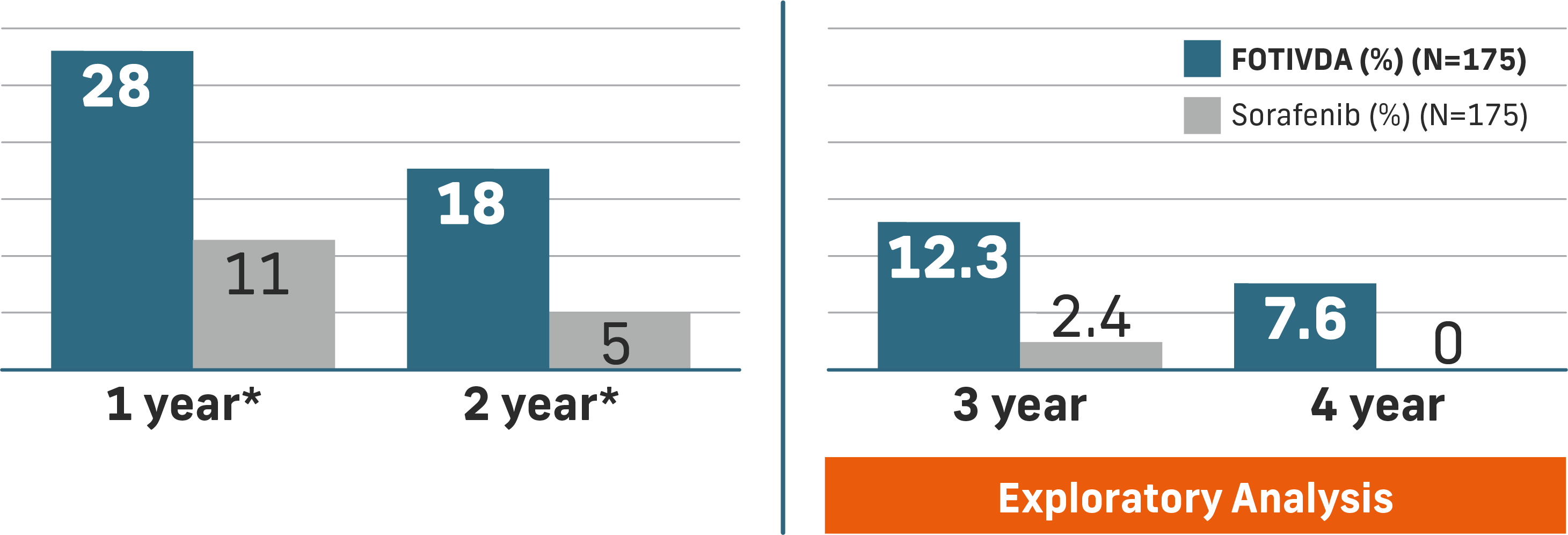
- LT-PFS data is based on exploratory analysis of investigator-assessed PFS, with a study start date of May 2016 and a date cutoff of May 24, 20211,3
- Investigator-assessed PFS analysis upon extended follow-up was consistent with the independent review committee PFS analysis, which was the primary endpoint for TIVO-33
- The safety profile of FOTIVDA was consistent with the full Prescribing Information
*Open-label, multicenter study in North America and the European Union. Primary endpoint: PFS assessed by blinded independent review committee. Secondary endpoint: ORR (defined as CR+PR), DOR, OS, tolerability, and safety.
Primary PFS endpoints for FOTIVDA
See Dr. Pedro C Barata, Director of GU Medical Oncology Research Program, University Hospitals Seidman Cancer Institute, talk about the value of FOTIVDA’s efficacy data.
FOTIVDA is the first and only VEGFR TKI with long-term PFS data in 3L RCC treatment.
Watch a discussion of the 3- and 4-year PFS data with Dr. Pedro C Barata in this short informative video.
See PFS analysis by subgroup.
Explore safety and tolerability.
Reach out to an AVEO Oncology Account Manager.
CI=confidence interval; CR=complete response; DOR=duration of response; HR=hazard ratio; LT=long-term; mPFS=median progression-free survival; ORR=overall response rate; OS=overall survival; PR=partial response.
References: 1. Rini BI, Pal SK, Escudier BJ, et al. Tivozanib versus sorafenib in patients with advanced renal cell carcinoma (TIVO-3): a phase 3, multicentre, randomised, controlled, open-label study. Lancet Oncol. 2020;21(1):95-104. 2. FOTIVDA (tivozanib) [package insert]. Boston, MA: AVEO Pharmaceuticals, Inc, January 2025. 3. Beckermann KE, Asnis-Alibozek AG, Atkins MB, et al. Long-term survival in patients with relapsed/refractory advanced renal cell carcinoma treated with tivozanib: analysis of the phase III TIVO-3 trial. Oncologist. 2024;29(3):254-262.
INDICATIONS AND IMPORTANT SAFETY INFORMATION
INDICATIONS
FOTIVDA is indicated for the treatment of adult patients with relapsed or refractory advanced renal cell carcinoma (RCC) following two or more prior systemic therapies.
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Hypertension was reported in 45% of patients (22% ≥ Grade 3). Hypertensive crises were reported in 0.8% of patients. Do not initiate FOTIVDA in patients with uncontrolled hypertension. Monitor for hypertension and treat as needed. Reduce the FOTIVDA dose for persistent hypertension not controlled by anti-hypertensive medications. Discontinue FOTIVDA for severe hypertension that cannot be controlled with anti-hypertensive therapy or for hypertensive crisis.
INDICATIONS
FOTIVDA is indicated for the treatment of adult patients with relapsed or refractory advanced renal cell carcinoma (RCC) following two or more prior systemic therapies.
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Hypertension was reported in 45% of patients (22% ≥ Grade 3). Hypertensive crises were reported in 0.8% of patients. Do not initiate FOTIVDA in patients with uncontrolled hypertension. Monitor for hypertension and treat as needed. Reduce the FOTIVDA dose for persistent hypertension not controlled by anti-hypertensive medications. Discontinue FOTIVDA for severe hypertension that cannot be controlled with anti-hypertensive therapy or for hypertensive crisis.
Cardiac failures were reported in 1.6% of patients (1% ≥ Grade 3); 0.6% of events were fatal. Monitor for signs or symptoms of cardiac failure during treatment with FOTIVDA. Manage with dose interruption, dose reduction, or discontinuation.
Cardiac ischemia were reported in 3.2% of patients; 0.4% of events were fatal. Arterial thromboembolic events were reported in 2.0% of patients, including death due to ischemic stroke (0.1%). Closely monitor patients at risk for, or who have a history of these events. Discontinue FOTIVDA in patients who develop severe arterial thromboembolic events, such as myocardial infarction and stroke.
Venous Thrombotic Events (VTE) were reported in 2.4% of patients, including 0.3% fatal events. Closely monitor patients who are at increased risk for these events. Discontinue in patients who develop serious VTEs.
Hemorrhagic Events were reported in 11% of patients; 0.2% of events were fatal. Use FOTIVDA with caution in patients who are at risk for or who have a history of bleeding.
Proteinuria was reported in 8% of patients (2% = Grade 3). Monitor during treatment with FOTIVDA. For moderate to severe proteinuria, reduce the dose or interrupt treatment. Discontinue in patients who develop nephrotic syndrome.
Gastrointestinal (GI) Perforation including fatal cases, has been reported in patients receiving FOTIVDA. Monitor for symptoms of GI perforation or fistula formation periodically throughout treatment with FOTIVDA. Permanently discontinue FOTIVDA in patients who develop severe or life-threatening GI perforation.
Thyroid Dysfunction events were reported in 11% of patients (0.3% ≥ Grade 3). Monitor thyroid function before and during treatment with FOTIVDA.
Wound Healing Complications: Withhold FOTIVDA for at least 24 days prior to elective surgery and do not administer for at least 2 weeks after major surgery and until adequate wound healing is observed.
Reversible Posterior Leukoencephalopathy Syndrome (RPLS) can occur with FOTIVDA. Evaluate for RPLS in patients presenting with seizures, headache, visual disturbances, confusion, or altered mental function. Discontinue if signs or symptoms of RPLS occur.
Embryo-fetal Toxicity: FOTIVDA can cause fetal harm. Advise patients of the potential risk to a fetus, to avoid becoming pregnant and to use contraception during treatment and for one month after the last dose of FOTIVDA. Advise males with female partners of reproductive potential to use effective contraception during treatment and for one month after the last dose of FOTIVDA.
Allergic Reaction to Tartrazine: FOTIVDA 0.89 mg capsule contains FD&C Yellow No. 5 (tartrazine) which may cause allergic-type reactions (including bronchial asthma) in certain susceptible patients.
ADVERSE REACTIONS
Common adverse reactions include fatigue/asthenia, hypertension, diarrhea, decreased appetite, nausea, dysphonia, hypothyroidism, cough, and stomatitis.
Serious adverse reactions include bleeding (3.5%), venous thromboembolism (3.5%), arterial thromboembolism (2.9%), acute kidney injury (2.3%), and hepatobiliary disorders (2.3%).
DRUG INTERACTIONS
Avoid coadministration with strong CYP3A4 inducers.
USE IN SPECIFIC POPULATIONS
Advise women not to breastfeed during treatment and for at least 1 month after the last dose.
The recommended dosage for patients with end-stage renal disease has not been established.
Reduce the FOTIVDA dose for patients with moderate hepatic impairment. The recommended dosage in patients with severe hepatic impairment has not been established.
To report SUSPECTED ADVERSE REACTIONS, contact AVEO Pharmaceuticals, Inc. at 1-833-FOTIVDA (1-833-368-4832) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please see full Prescribing Information for FOTIVDA® (tivozanib).
